When PD progresses, increasing GOOD ON time can help alleviate the burden of motor complications
As the therapeutic window of levodopa narrows during PD progression, daily disruptions become more frequent and unpredictable1,2

of patients with PD experience OFF, dyskinesia, or both within 5 years after starting levodopa3
Widening the therapeutic window by simultaneously treating both OFF time and dyskinesia can increase patients’ overall GOOD ON time1,2,4

Increasing GOOD ON time had a direct positive impact on patients’ daily lives
With more GOOD ON time, patients observed the following changes*,5-7
More independence in performing activities of daily living
Fewer uncontrolled
motor symptoms
Fewer disruptions while in a public or social setting
*There are no studies showing that GOCOVRI affects specific outcomes above.
When motor complications occur, it may be beneficial to consider adding an NMDA, N-methyl-D-aspartate, antagonist (glutamatergic pathway) to complement the current dopaminergic treatment regimen.*,8
*The mechanism by which amantadine exerts efficacy in the treatment of dyskinesia and OFF time in patients with PD is unknown.4

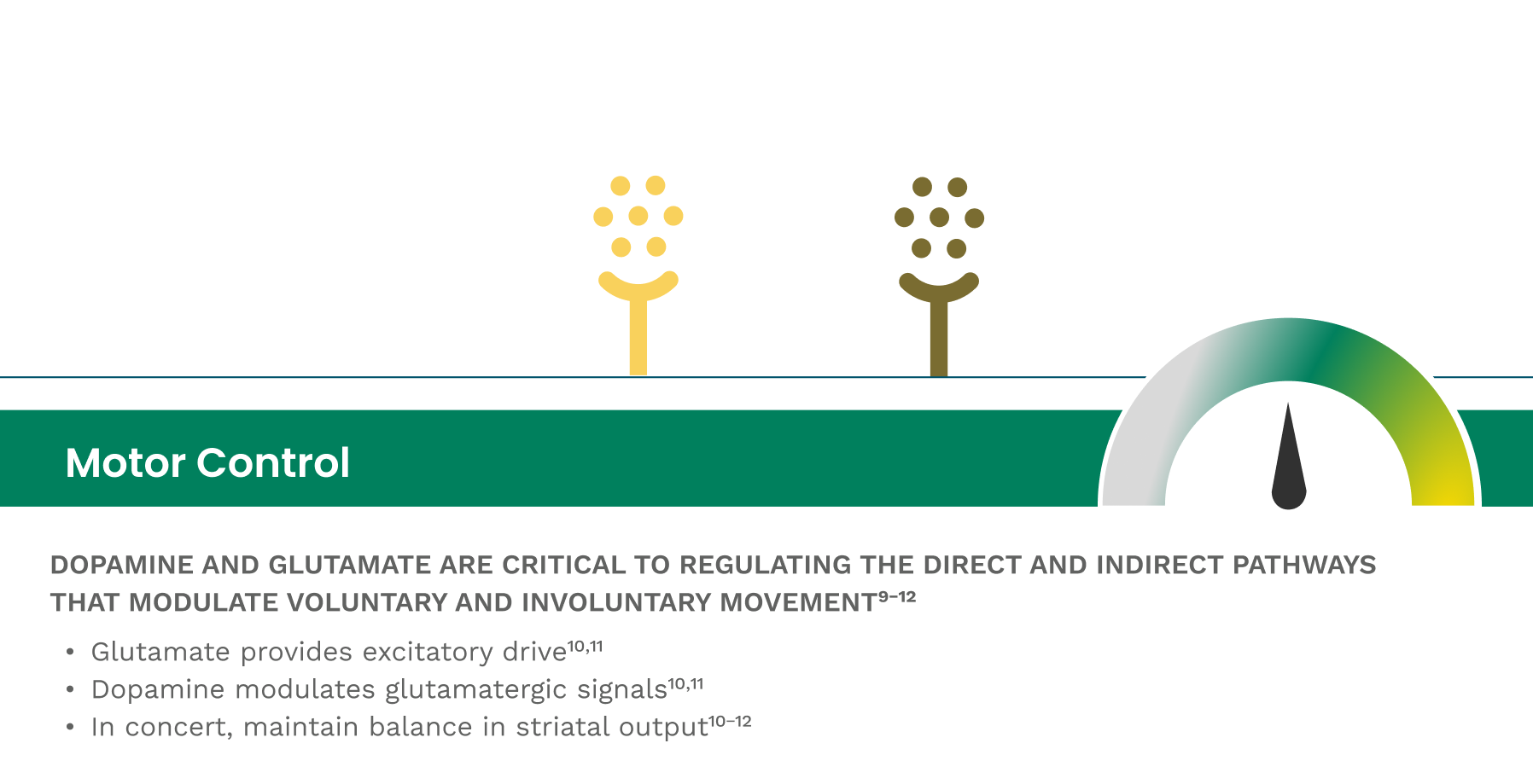
Understanding the role of glutamate in PD
Dopamine is only part of the story when it comes to controlling motor complications.8
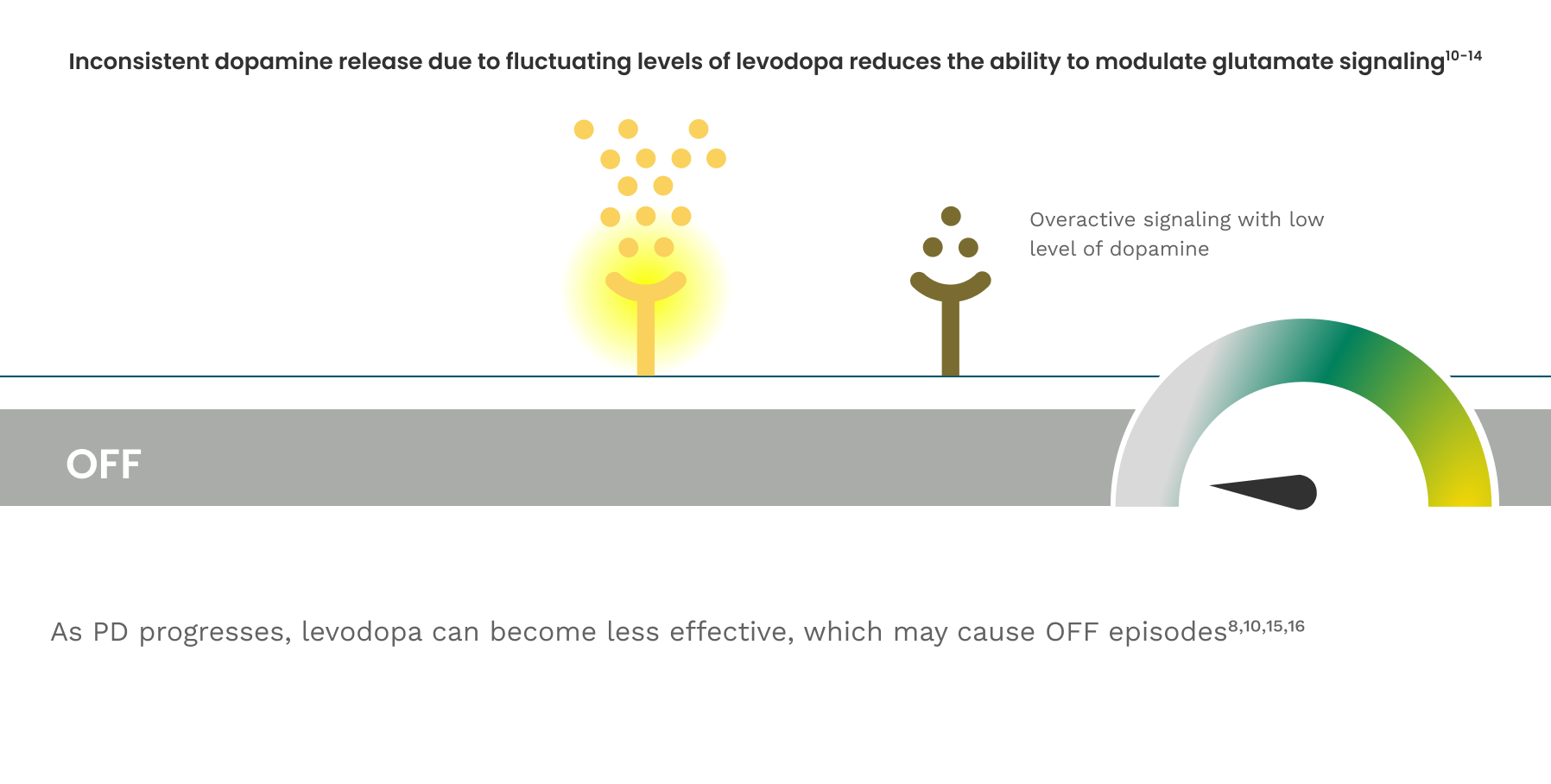
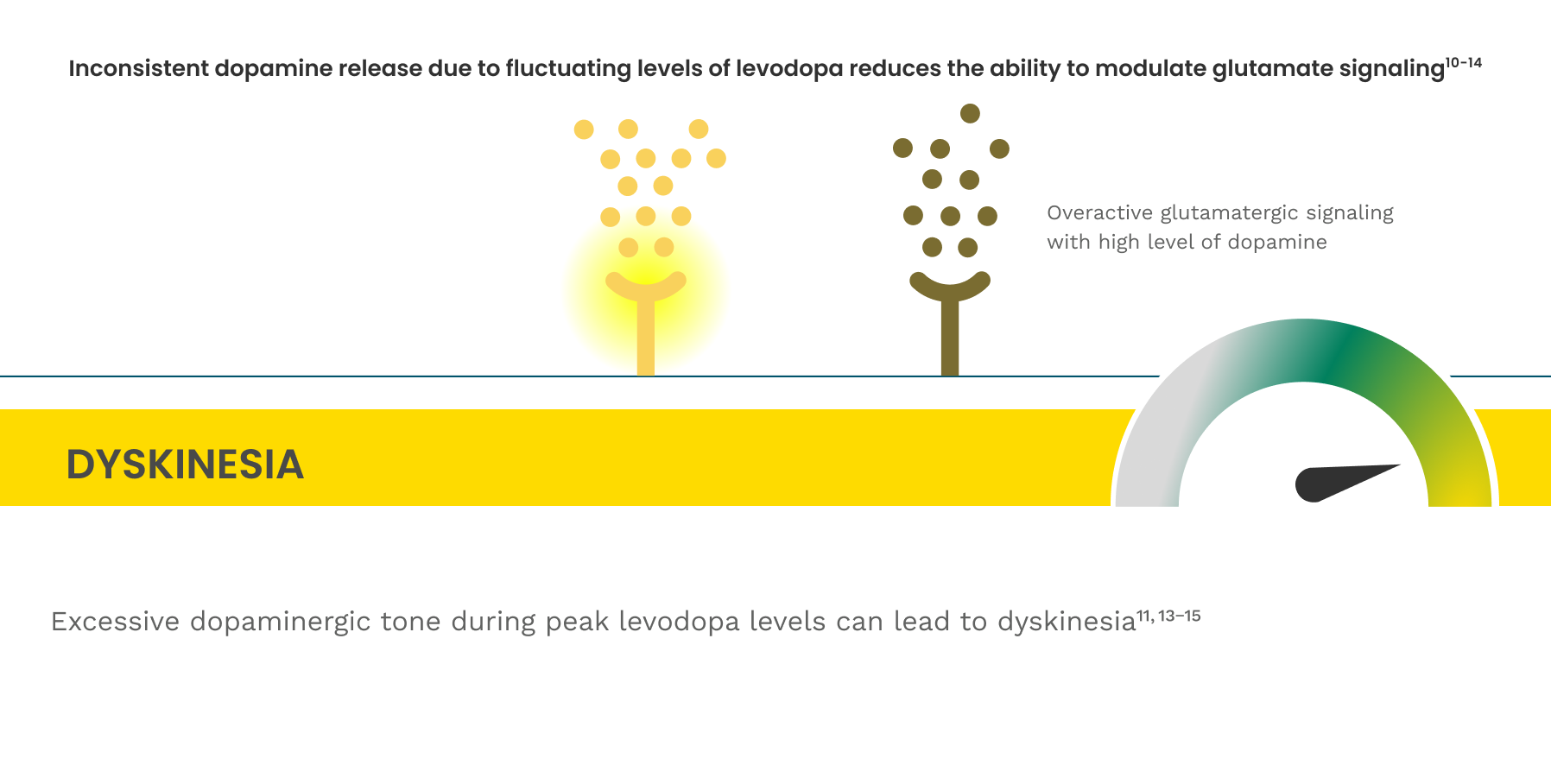
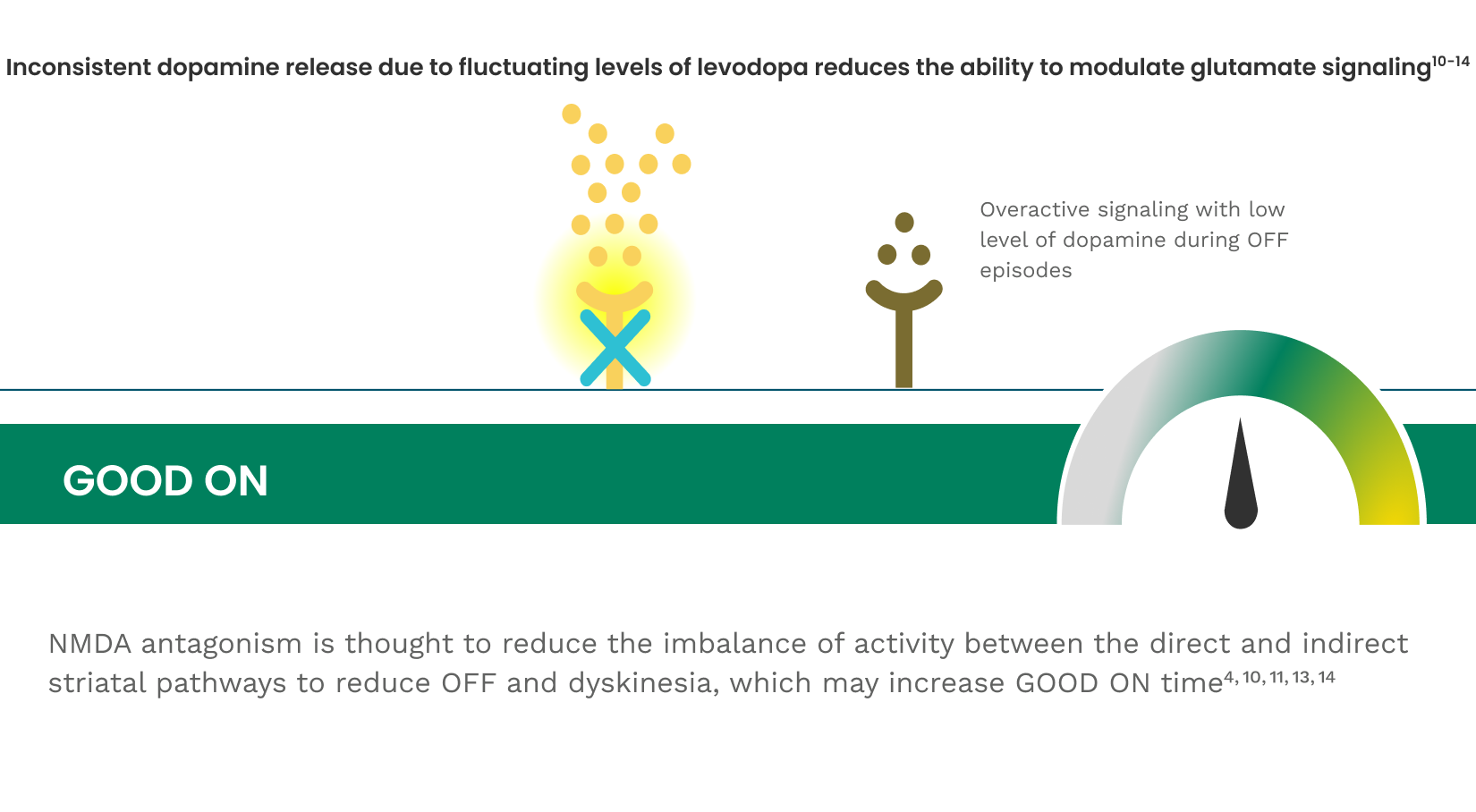
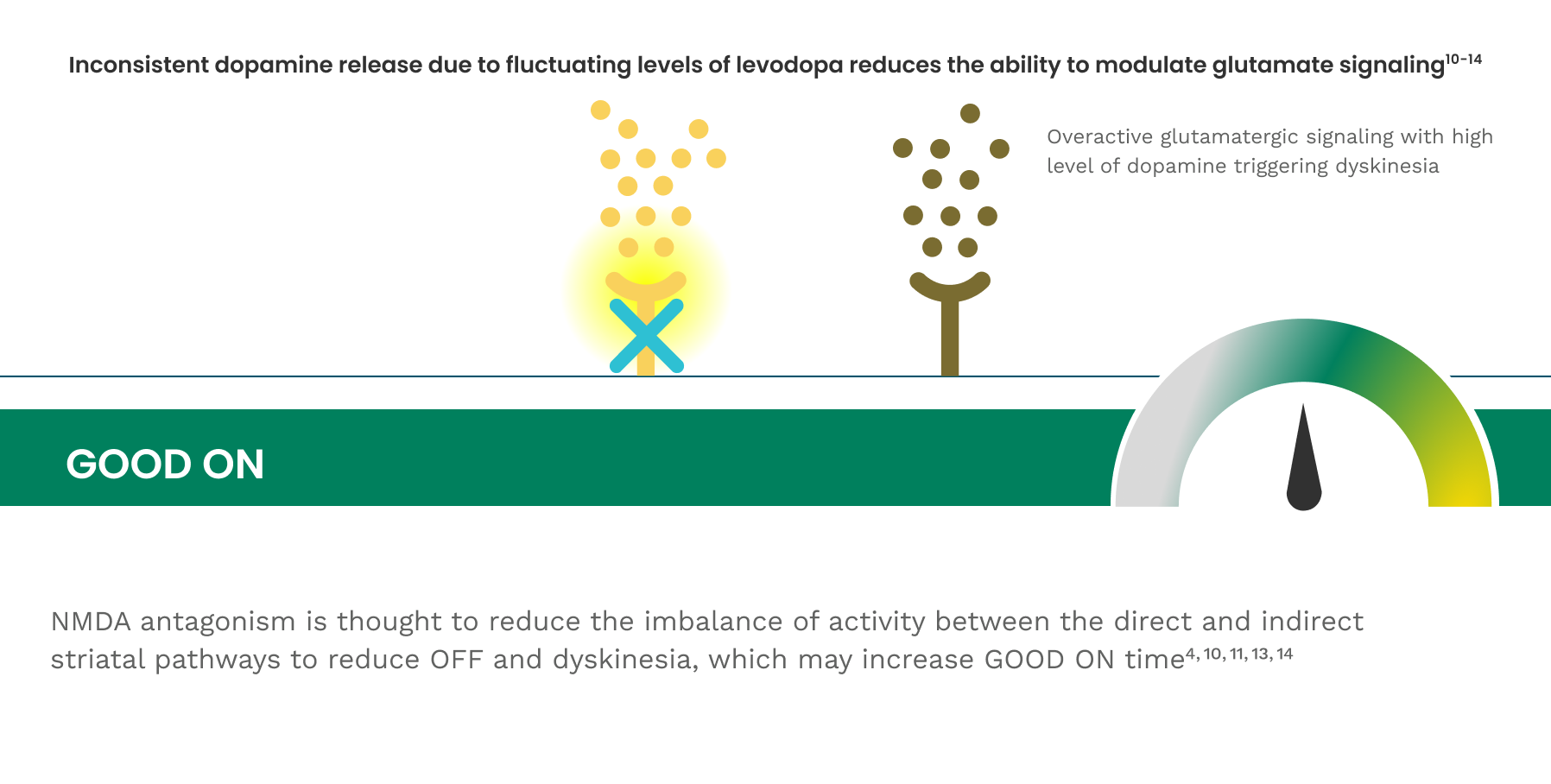
Reducing glutamate hyperactivity through the NMDA receptor could be critical to reducing dyskinesia and OFF time†,8
NMDA. A synthetic amino acid C5N9NO4 that binds selectively to a subset of glutamate receptors on neurons.17
†The mechanism by which amantadine exerts efficacy in the treatment of dyskinesia and OFF time in patients with PD is unknown.4
How amantadine is believed to work
AMANTADINE IS AN NMDA ANTAGONIST USED IN PD TREATMENT‡,18,19
- Amantadine is used for symptomatic treatment for PD and can reduce levodopa-induced dyskinesia and OFF time.18,21,22
- GOCOVRI is the only formulation of amantadine proven to reduce both dyskinesia and OFF time.4
- Amantadine IR is not indicated for reducing OFF time.18
- The mechanism by which amantadine exerts efficacy in the treatment of dyskinesia and OFF time in patients with PD is unknown.4
- May work by reducing excessive glutamatergic activity, which contributes to dyskinesia and OFF time.10
- Amantadine may have direct and indirect effects on dopamine neurons; it exerts dopaminergic-like side effects such as hallucinations and dizziness in humans.18
- Common daily dosing of amantadine HCl IR in PD is 100 mg BID.18

‡Amantadine is a low-affinity, noncompetitive NMDA antagonist, which means inhibition of the NMDA channel occurs at a different binding site than the active site where the substrate binds.18-20
Get the conversation going about motor complications

Managing dyskinesia and OFF time begins with a discussion among you, your patient, and their care partner.
Your patients may not always be forthcoming about the difficulties they face with dyskinesia and OFF time. There are many reasons for this behavior. Keep in mind that your patients may:
- Downplay their dyskinesia to avoid OFF time
- Not realize the impact or effects of their dyskinesia or OFF time
- Believe dyskinesia is just a sign of disease progression
- Assume there are no dyskinesia treatment options
The following may indicate that your patients struggle with dyskinesia and OFF time:
- They make comments that imply compromise or settling
- Describing unpredictable episodes of dyskinesia, ON, and OFF time
- Referring to ON time negatively
- An increase in "accident prone" behaviors
- Difficulties with activities or hobbies
- Feeling embarrassed in social situations
- Care partner makes comments about movement control
- Difficulties at work

Download our discussion guide
Have your patients fill it out to give you a better understanding of how dyskinesia and OFF time are impacting their day.
What efficacy data does GOCOVRI have?
GOCOVRI is backed by 2 Phase 3 clinical trials. These studies assessed the ability of GOCOVRI to reduce dyskinesia (primary endpoint), reduce OFF time (secondary endpoint), and increase GOOD ON time (secondary endpoint).4,22,23
Get clinical information on GOCOVRI
Get the latest news and updates about GOCOVRI®, learn about upcoming events, and more.