GO with less dyskinesia, less OFF time, and more GOOD ON time
JUMP TO SECTION
Robust clinical program consisting of 2 Phase 3 studies and a long-term open-label extension (OLE) study1-4
The efficacy and safety of GOCOVRI 274 mg QHS were evaluated in 2 Phase 3, randomized, placebo-controlled trials:
Study 11,3,5
24-week study
121 PD patients* with dyskinesia GOCOVRI (n = 63), placebo (n = 58)
Study 22,3,5
12-week study
75 PD patients* with dyskinesia GOCOVRI (n = 37), placebo (n = 38)
Study design
- Phase 3 randomized, placebo-controlled
- 274 mg GOCOVRI®, QHS
- Baseline PD medications including levodopa were held constant
Primary endpoint
- Change in UDysRS† total score from baseline to week 12
Secondary endpoints
- Change from baseline to week 12 in ON time without troublesome dyskinesia and OFF time based on patient home diary data
Long-term open-label study4
100 weeks, N = 223
- Open-label
- 274 mg GOCOVRI®, QHS
- Adjustments to baseline PD medications including levodopa were allowed
- Evaluated long-term safety, and tolerability
*Patients who had at least 1 hour of troublesome dyskinesia time during the day and at least mild functional impact because of dyskinesia.5
†The Unified Dyskinesia Rating Scale (UDysRS) is a standardized clinical research tool that uses both patient historical and objective measurements to assess presence of dyskinesia and its impact on daily activities. Total scores range from 0 to 104 points, with higher scores indicating more severe dyskinesia.6
Dyskinesia = ON time with troublesome dyskinesia.
Pooled Studies at Baseline3,5
UDysRS total score:
40.1
points (mean)
ON time with troublesome dyskinesia:
4.9
hours (mean)
OFF time:
2.8
hours (mean)
GOOD ON time:
8.4
hours (mean)
GOOD ON time = ON time without troublesome dyskinesia.
DYSKINESIA ENDPOINT (PRIMARY)3
41% improvement in dyskinesia with GOCOVRI® (in UDysRS from baseline) without adjustments to existing dopaminergic medications3,7
Pooled results: mean improvement in UDysRS total score at week 12 (mean baseline of all patients, 40.1)3,7
‡Percent improvement from baseline calculated using MMRM statistics model.3
Adapted from Elmer et al.
OFF TIME ENDPOINT (SECONDARY)§,3,7
21% reduction in OFF time with GOCOVRI® (from baseline) without adjustments to existing dopaminergic medications3,7
Pooled results: mean reduction in OFF time at week 12 (mean baseline of all patients: 2.8 hours)3,7
§Derived from patient diary data.
Adapted from Elmer et al.
SECONDARY ENDPOINT||,3
+3.8-hour increase in GOOD ON time with GOCOVRI® (from baseline) without adjustments to existing dopaminergic medications¶,#,3,7
Pooled results: mean increase in GOOD ON time at week 12 (mean baseline of all patients: 8.4 hours)3,7
||Derived from patient diary data.
¶GOOD ON time = ON time without troublesome dyskinesia. All patients, including those taking placebo, were on a stable regimen of anti-Parkinson’s disease medication.3
#Pooled patient diary results from studies 1 and 2 at 12 weeks.1-3
Adapted from Elmer et al.
More GOOD ON time throughout the day due to reductions in both dyskinesia and OFF time3,7,8
Increased GOOD ON time: results from pooled patient diary data at week 127,8
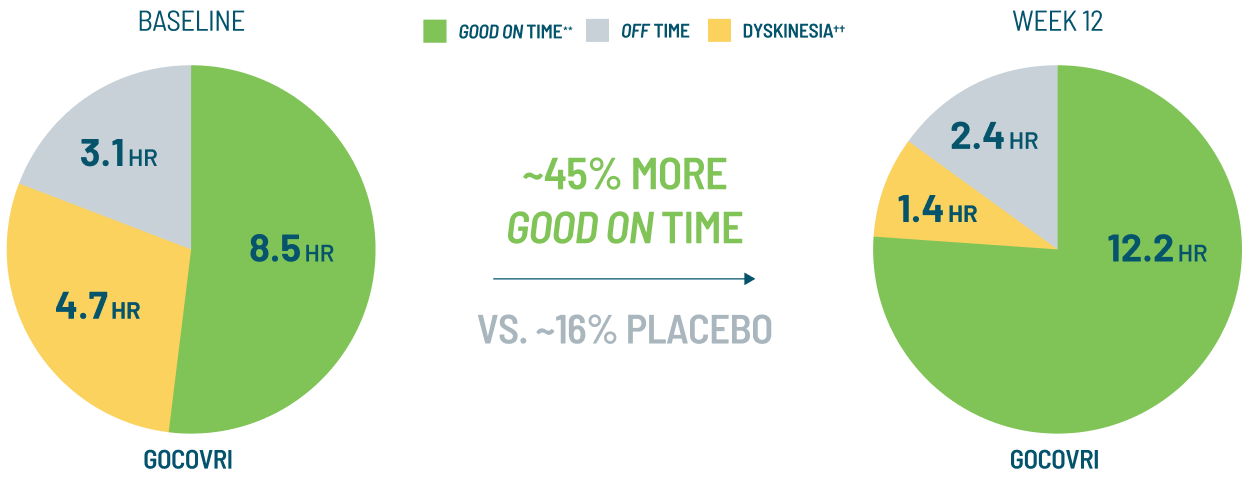
Pooled placebo values (hours) for dyskinesia, OFF time, GOOD ON time, at baseline and Week 12, respectively: 5.2, 2.6, 8.1, and 3.1, 3.1, 9.6.
**GOOD ON time = ON time without troublesome dyskinesia.
††Dyskinesia defined as ON time with troublesome dyskinesia.
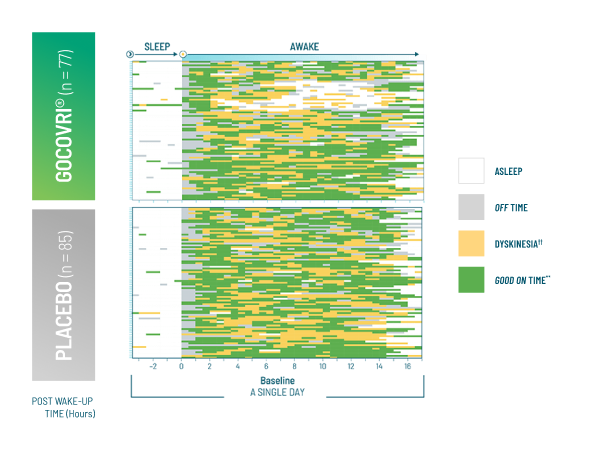
RESULTS FROM A POST-HOC ANALYSIS OF DIARY DATA
Exploring whether reductions in daily episodes increased continuous GOOD ON time9
Sample diary plot for a single patient throughout the waking day9

**GOOD ON time = ON time without troublesome dyskinesia.
††Dyskinesia defined as ON time with troublesome dyskinesia.
RESULTS FROM A POST-HOC ANALYSIS OF DIARY DATA
Exploratory analysis assessed the impact of GOCOVRI on dyskinesia and OFF time on continuous GOOD ON time9
Post-hoc analysis of patient diary plots (N = 162) representing 1 day at baseline and week 12‡‡,9
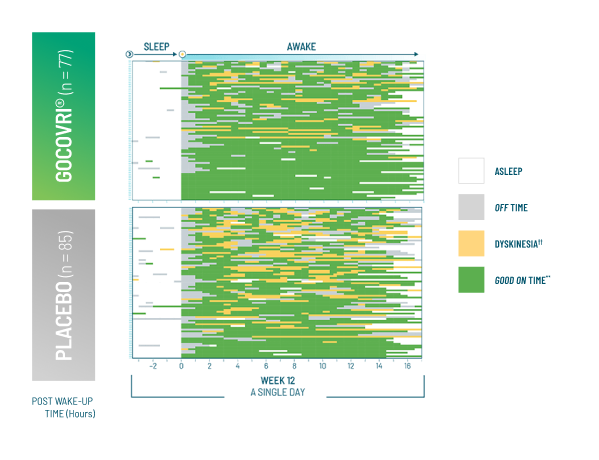
Adapted from Hauser et al.
**GOOD ON time = ON time without troublesome dyskinesia.
††Dyskinesia defined as ON time with troublesome dyskinesia.
‡‡Patients are organized in descending order of number of episodes reported at Week 12 (with baseline reordered to match, so that patient order is the same at baseline and Week 12).9
AT WEEK 129:
57.1%
of patients receiving GOCOVRI reported no episodes of dyskinesia (vs. 24.7% with placebo)
27.3%
reported no OFF time (vs. 20.0% with placebo)
19.5%
reported no dyskinesia nor OFF time (vs. 3.5% with placebo)
A retrospective, subgroup analysis of patient diary data9:
- Included only patients with baseline and Week 12 diaries (n = 162/196)
- Evaluated the frequency, prevalence, and duration of episodes of troublesome dyskinesia and OFF time
- Analyzed the effect of GOCOVRI® on these episodes
- Episodes are defined as time spent in a PD diary motor state (dyskinesia or OFF time) before entering another state
Limitations of this analysis9:
- Only analyzed preexisting data derived from a population with at least mild dyskinesia at baseline
- Did not include patients who withdrew from the study prematurely
- Did not include tools for capturing the intensity of clinical states
Due to these limitations, this analysis may not be applicable to a more generalized PD population, and no formal conclusions can be drawn.
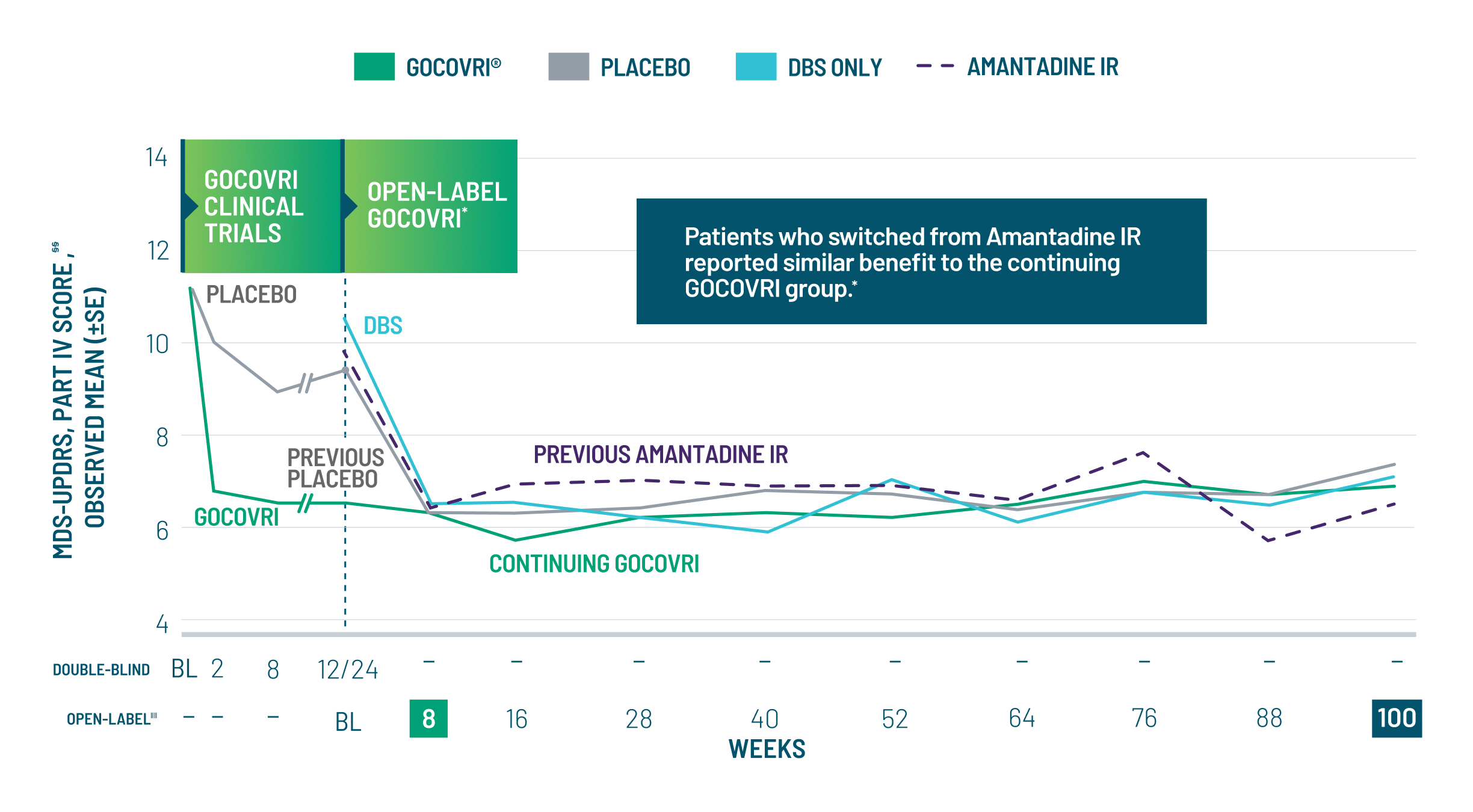
Reductions in motor complication scores were maintained for all groups, regardless of previous therapy, for the full 2 years of the OLE4,10
This study's real-world design permitted treatment with and adjustment of concomitant PD treatments. The lack of a blinded control group reduced the certainty that study findings were due to GOCOVRI. No formal comparisons can be made between GOCOVRI and other treatment regimens.
MDS-UPDRS Part IV measures motor complications within the last week, including:
- Time spent with dyskinesia (0-4 pts)
- Functional impact of dyskinesia (0-4 pts)
- Time spent in OFF dystonia (0-4 pts)
- Motor fluctuations:
- Time spent in motor fluctuations (0-4 pts)
- Functional impact of motor fluctuations (0-4 pts)
- Complexity of motor fluctuations (0-4 pts)
Hear OLE Insights From
Dr. Kremens
§§MDS-UPDRS Part IV captures changes in dyskinesia and OFF symptoms with a higher score, indicating an increase in severity (maximum score of 24).
‖‖Number of patients enrolling directly from the double-blind were at baseline and at week 100, respectively: continuing GOCOVRI 60, 37; previously on placebo: 78, 42; DBS: 61, 41; previously on amantadine IR: 32, 20.
What safety data does GOCOVRI have?
Take a closer look at the safety profile of GOCOVRI outlined in the Phase 3 clinical trials and the long-term OLE study.
Get clinical information on GOCOVRI
Get the latest news and updates about GOCOVRI®, learn about upcoming events, and more.